
Model of Psychological Needs
According to Schema Therapy psychopathological symptoms can be best understood by frustrated psychological needs that are depicted below:
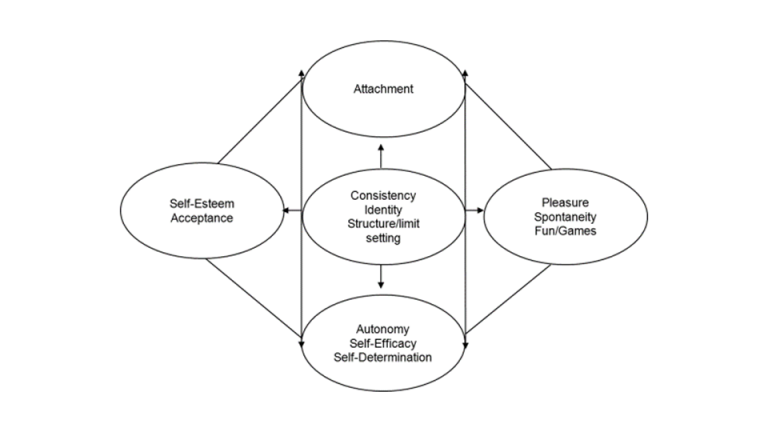
(based on Loose, Graaf, & Zarbock, 2013, modified from Grawe, 2017)
Early Maladaptive Schemas (EMS)
Four types of early life experiences can be differentiated that can lead to the development of a schema:
- Continuing/ toxic frustration of emotional needs (too little of a good thing)
- Traumatization or victimization (the child is harmed or victimized)
- Overprotection (too much of a good thing)
- ”Overload“ of adult themes (e.g. parentification after divorce)
References:
Young, J.E., Klosko, J. S., Weishaar, M. E. (2006). „Schema Therapy: A Practitioner’s Guide. New York/London: Guilford Press
Coping Styles
Avoidance: finding ways to escape or block out schemas as a protection. Children using this strategy appear distant, it is hard to get a feeling for them, and they appear as if they were sitting behind a glass wall.
Surrender: giving in to schemas and repeating them over and over. Your perception of the world can be biased by your negative expectations. This strategy leads to a reduction of inner tension based on the notion: „that‘s me“ (ego-syntonic). Nevertheless, the degree of internal suffering usually remains high.
Overcompensation: doing the opposite of what the schemas make you feel. Again, the perception is often biased to enhance one’s self-esteem (self-serving bias; („I knew it before“). Children may appear self-confident and autonomous, while being fragile and easily confused. Usually, the caregivers indicate a higher degree of suffering than the children.
The dominant coping style of children depends on their temper, learning experience and significant role models (e.g. father, mother, sibling, peers, etc.).
Reference:
Rafaeli E., Bernstein, D.P. , Young, J.E. (2011). Schema Therapy. The CBT Distinctive Features Series. New York: Routledge.
Modes & Mode Work
Schema modes are emotional states at a given point of time, triggered by life situations the person is oversensitive to („emotional buttons“). While these states are each associated with a schema, it is not possible to allocate them 1-to-1. A schemarepresents a trait, and a mode is comparable with a state.
There are 4 main types of modes I-II-III-IV (including subgroups A,B,C …):
I. Child modes: „The little …[name of the child]“
II. Demanding and punishing modes: „The critical … [name of the child]“
III. Immature coping modes: „Emergency-… [name of the child] “
IV. Clever-mode: „The clever …[name of the child] “
In therapy with adults this mode is called the healthy adult mode. Of course, a child is not an adult, therefore we renamed this healthy mode “the clever ..“ (name of the child).
Important: It is recommended to avoid talking of „parent modes“, because a conflict of loyalty could occur hindering the child from building up a trusting relationship to the therapist.